In PRI Vision, we spend our clinical days helping patients gain the ability to center themselves in space. We define centering as the neurological ability to use appropriate visual perception, capitalize on ascending support, and balance on each side. To center correctly, you must be able to be “neutral” as defined by PRI while performing this task. However, a person can be “neutral” and still not be able to center. Even though we are using visual input through the eyes to help patients accomplish this, centering must start with the floor.
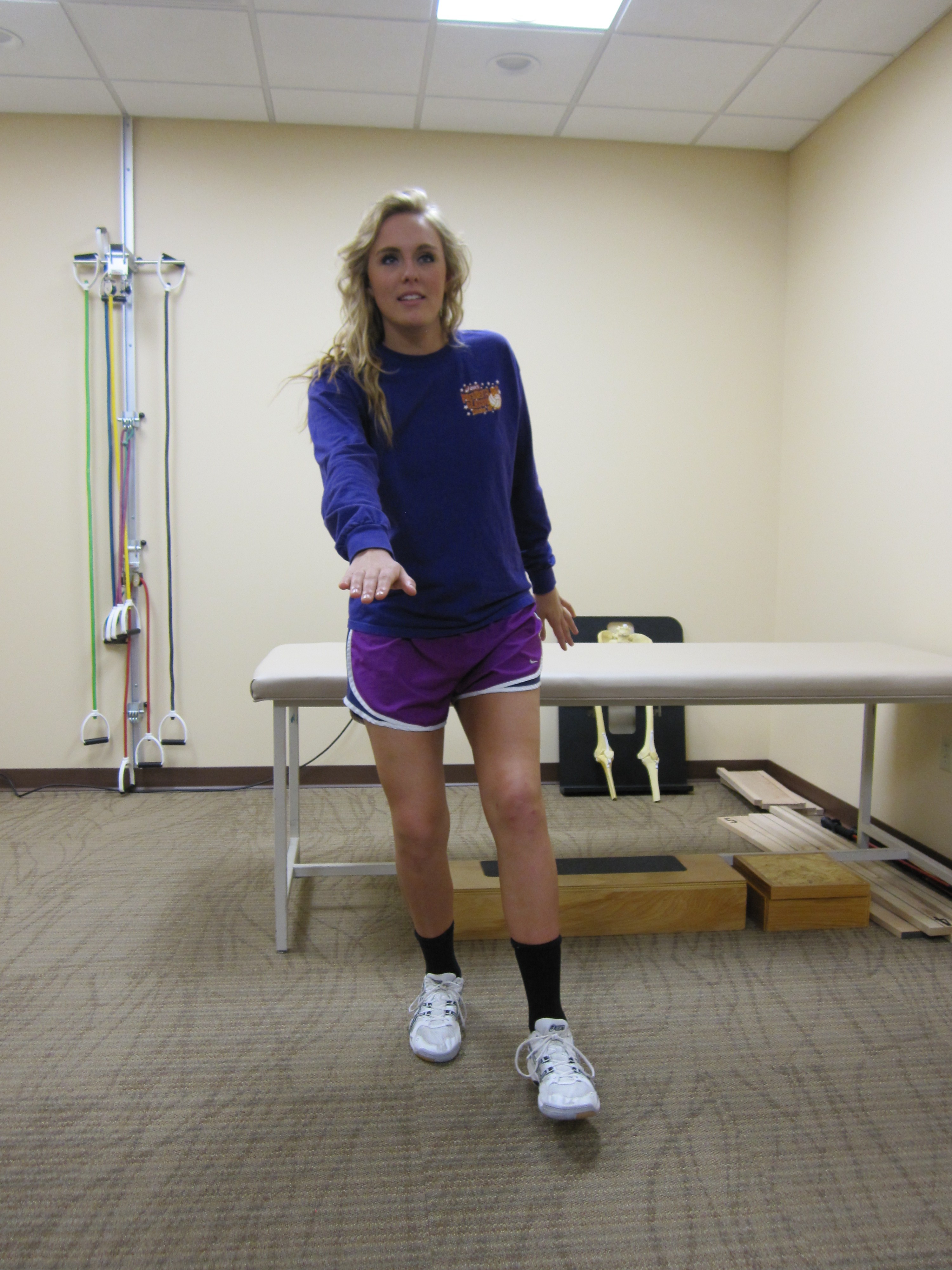
Poor Right Centering with Extension; note how the trunk is fairly straight, rather than flexed, evidenced by lack of side-bending at the waist and from the side view by a flat back. The whole trunk is leaning to the right with the left leg as counter-balance for the trunk.

Appropriate Right Centering with Flexion; note how there is a side-bend in the trunk, showing right abdominal engagement for trunk support, rather than the left leg utilized for this purpose. Her nose lines up well to the right of her midline without head tilting to accomplish this. From the side view, rounding of the back would be observed, further indicating flexion of the trunk.
Sensory awareness of the floor may seem like an overly simple thing to possess. We have the patient attempt to center themselves, and then ask them what they feel holding them up. Especially when on only one leg, many of our PRI VIsion patients can’t answer that question; some of our patients can answer it when on one side, the right for instance, but not when on the left. The reality is that they really don’t know what muscles they are using. Some might answer their ankle, knee, back, or even their neck. Others are concentrating very hard and staring at the ground to help them balance, effectively using muscles around the eyes to help them stabilize themselves; this is another inappropriate substitute for poor sensory floor awareness. All of these floor-challenged patients have ceased to use the floor for ascending support; instead of pushing down on the floor to fight gravity, they are using extension muscles to pull themselves away from the floor and gravity. The heel, arch, inner thigh, outer hip, and abdominal muscles, important reference centers in the world of PRI, are not engaged, nor can they find them to activate them even when thinking about it.
The more disconnected a person is from the floor for proprioception and sensory input, the greater the chance that they have overactive neck muscles and associated symptoms. On the lesser end of the spectrum, they may have neck and/or back tension. At the more involved end of the spectrum they can also experience dizziness or disorientation, tachycardia, lightheadedness or fainting, and shortness of breath. In these more involved patients, tension in muscles associated with extension activity is so chronic that it takes the place of appropriate reference centers. Shutting down those muscles may make the patient actually feel worse until they are able to find, or are given, new references, and can meaningfully use them.
The concept of using the floor for support, neurologically-speaking, is not new to PRI. The right arch and left heel are some of the first references taught in PRI to help gain and maintain PRI-defined neutrality. In PRI Vision, the basis for this concept is taken from AM Skeffington’s (the father of behavioral optometry) description of vision that was written in the middle of the last century. In it, he states that every 250 milliseconds, a process takes place that begins with coming to balance with gravity, uses information about the space around you from the eyes, and results in vision as the “emergent” from the process. In other words, how our vision behaves has to start with our body (and really, the brain), first dealing with gravity. The space around you is literally the air and objects around, under, and above you. It then stands to reason that the better we can deal with gravity the right way and make sense of the space we are in, the more efficient and less taxed our visual process can be.
Ideally, we should be able to balance on one side without over-extending the body, unconsciously using appropriate references, and maintain this while freely moving our eyes around to any desired object; this demonstrates good ability to center. When a patient is overusing the visual system to do this, changes in the visual process happen. It could be that they tend to “fixate”, or stare, at one point to balance, as in the above example of staring at the floor. A more commonly-seen change in PRI Vision is that the patient can’t alter the way they are attempting to center themselves until we alter the space around them through lenses.
What does this mean in terms of treating patients everyday? We don’t claim to have all the answers. But we do believe that the more aware a patient is of the floor, especially on the left after an activity that helps them become neutral, the more likely they are to maintain that neutrality. Conversely, if they have poor floor awareness, or it’s not at least equal on the left to that on the right, you need to look further up the muscle chains for a descending problem.
At the top of all the chains taught in PRI, is vision. Not every patient who needs PRI Vision intervention has poor floor awareness. But if a patient is not able to find awareness of the floor, even if momentarily “neutral”, they will likely need PRI Vision intervention to see it differently, so that they may find the floor and keep it without challenging the visual process to do so.
As Always, Keep Moving Beyond Sight!
Dr. Heidi
